|
Overview
 Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients. Causes Most commonly fallen arches in adulthood can arise due to Posterior Tibial Tendon Dysfunction (PTTD). The posterior tibial tendon plays a pivotal role in holding up the arch of the foot, damage to this tendon results in the arch collapsing. Another cause of acquired flat feet in adulthood may be due to Rheumatoid arthritis as this disease attacks the bone, cartilage and ligaments in the foot causing it to change shape and flatten. Injury to the ligament, fracture and/or dislocation of the bones in the mid foot can all lead to a flat foot deformity. Adult acquired flat fleet can also arise in people who have diabetes or a neurological condition which limits normal feeling in the foot, the muscles in feet switch off, the tendons and ligaments weaken, and the arch eventually collapses. Symptoms Not everyone who has flat feet experiences symptoms. Others, however, feel persistent pain in their feet and wearing shoes can prove additionally painful. Others only feel symptoms when they walk more than normal, go jogging or participate in a sport that involves running or kicking. Diagnosis You can always give yourself the ?wet test? described above to see whether you have flat feet. Most people who do not notice their flat feet or have no pain associated with them do not think to see a foot doctor. Flat feet can lead to additional problems such as stiffness or pain, however, especially if the condition appears out of nowhere. If you think you may have flat feet, you should seek medical attention to ensure there are no additional issues to worry about. Your doctor will be able to diagnose you with a number of tests. For example, he or she may have you walk around, stand still, or stand on your tiptoes while you are being examined. Your doctor may also examine your foot?s shape and functionality. It?s important to let your foot doctor know about your medical and family history. In some cases, your doctor may order imaging tests such as x-rays or an MRI (magnetic resonance imaging) to determine a cause of your flat foot. If tarsal coalition is suspected in children, a CT scan is often ordered. heelsncleavage Non Surgical Treatment Ligaments hold up arches. Deformed ligaments will not return to their original shape, just as an overstretched rubber band remains elongated. Arch supports help restore more normal function. Not all orthotics are made alike. Sole Supports custom designed orthotics are unique in the way they are cast. Sole Supports compensate for the differences between each foot. They take into account your body weight and the degree of flexibility in your feet. Taking care of fallen arches can be key in dealing with unresolved or recurrent back pain. Surgical Treatment  A combination of surgical procedures can be used to reconstruct the flatfoot. Generally, these procedures can be separated into those that correct deformities of the bones and those that repair ligaments and tendons. Your orthopaedic surgeon will choose the proper combination of procedures for your foot. Surgery of the foot can be performed under regional anesthesia, which is numbing the foot and ankle with a nerve or spinal block, or general anesthesia, which may require a breathing tube. A nerve block is often placed behind the knee to reduce pain after surgery. Prevention Sit up straight in a chair with your feet flat on the ground. Scrunch up the toes of one foot as if you are trying to grab hold of the floor then use your toes to drag your foot a small distance forwards. Do this a couple of times on each foot, but don?t use your leg muscles to push your foot forward -- the movement should come solely from the muscles in your feet. Sit in a chair and place a cleaning cloth, towel or small ball on the floor at your feet. Use the toes of one foot to grasp the object and lift it off the floor. This action will require you to clench your toes and contract your arch. Once you have lifted the object a little way off the floor, try to throw it in the air and catch it by stretching your toes and arch out and upwards. Repeat the exercise several times on both feet. Sit on the floor with your legs straight out in front of you then bend your knees out to either side and place the soles of your feet together so your legs form a diamond. Hold on to your ankles and, keeping your heels together at all times, separate your feet so your toes point out to either side. Open and close your feet in this way several times, making sure your little toes stay in contact with the floor throughout the exercise. Starting in the same position, try separating your heels, keeping your toes together at all times. After Care Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon. Overview
Every person?s body is unique and will show different symptoms due to a short leg. Athletes are able to distinguish the negative effects of a leg length that is just 3 mm shorter then the other. A whole host of negative effects can occur to the body that can create chronic pain and may necessitate surgical interventions. The effect of a short leg can be seen almost everywhere in the body.  Causes LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio. Symptoms Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side). Diagnosis On standing examination one iliac crest may be higher/lower than the other. However a physiotherapist, osteopath or chiropractor will examine the LLD in prone or supine position and measure it, confirming the diagnosis of structural (or functional) LLD. The LLD should be measured using bony fixed points. X-Ray should be taken in a standing position. The osteopath, physiotherapist or chiropractor will look at femoral head & acetabulum, knee joints, ankle joints. Non Surgical Treatment Heel lifts and sole lifts are simple ways Pedorthists can compensate for leg length deficiencies. These small modifications can make a tremendous difference to a person?s comfort, balance and mobility. Although people do not always know if they have LLD if you have any of the symptoms I have mentioned you should consult a Pedorthist as treating your condition early will reduce the development of serious problems later on.  shoe lifts for men's shoes Surgical Treatment Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces. Overview
 Heel pain is one of the most common conditions to affect the foot. It is usually felt as an intense pain when the affected heel is used. The pain is usually worse when you get out of bed in the morning or after a long period of activity. In most cases, only one heel is affected. After walking, the pain usually improves. However, it is common for it to be painful when you first take a step after a period of rest. The pain often worsens by the end of the day. Most cases of heel pain are caused by damage and thickening of the plantar fascia. Sometimes, the surrounding tissue and the heel bone also become inflamed (swollen). Causes There are many causes of heel pain. However, plantar fasciitis, also known as heel spur syndrome, is the most common, by far. The pain is usually localized to the bottom of the heel towards the inside of the foot. The arch may also be painful. With this condition, pain is typically most severe with the first few steps after a period of rest. The pain my then subside and then return after extended periods of standing. There is usually no specific traumatic event that is responsible for the condition. It is usually the result of overuse, e.g. too much standing, walking or running. There are several common contributory factors such as weight gain, foot type, shoes. Flat shoes or going barefoot are the worst. Athletic shoes are usually the best. The plantar fascia is a fibrous band or ligament that connects the ball of the foot with the heel and helps to support the arch. When this band gets stretched too much or overused, inflammation results, often at the location where it attaches to the heel bone. A heel spur may develop as a result of chronic pulling by the plantar fascia. However, it should be noted that the pain is not caused by the spur. In fact, in some of the most severe cases, there is no spur at all. In other instances, an X-ray may be taken for an unrelated condition and an extremely large but non-painful spur may be seen. Other causes of heel pain include gout, stress fracture, bone tumors, nerve entrapment and thinning of the fat pad beneath the heel. Pain at the back of the heel is usually not plantar fasciitis. (Pain at the back of the heel is often due to an inflammation of the Achilles tendon, enlargement of the heel bone or bursitis.) Symptoms Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment. Diagnosis A podiatrist (doctor who specializes in the evaluation and treatment of foot diseases) will carry out a physical examination, and ask pertinent questions about the pain. The doctor will also ask the patient how much walking and standing the patient does, what type of footwear is worn, and details of the his/her medical history. Often this is enough to make a diagnosis. Sometimes further diagnostic tests are needed, such as blood tests and imaging scans. Non Surgical Treatment The proper treatment for your heel pain depends entirely on the specific cause(s) of your symptoms. Therefore, it is critical to understand the cause(s) of your symptoms before beginning any treatment program and if you are unsure, then seeking medical advice is essential to develop the proper treatment program for your condition. Some common treatments are listed and can be performed at home. Keep in mind that not all of these treatments are appropriate for every condition, but they usually a good place to start. Rest, reducing activities for a few days can help to reduce the most severe pain. Ice, applying ice to the heel for 10 minutes several times a day will help to reduce inflammation. Stretching exercises, to lengthen the muscles in the back of the leg, including the hamstrings, will help to ease pain, reduce focal pressures to your feet and assist in recovery. For plantar fasciitis, this may be the best treatment of all. Avoid going barefoot, when without shoes excessive stress and strain is placed on the plantar fascia. Proper shoe gear, supportive shoes that fit and are not too worn along with good arch support help to reduce the stress and strain on the plantar fascia over time. Medications, non-steroidal anti-inflammatory medication, such as Motrin (ibuprofen), may help to reduce inflammation. If the pain persists or worsens after a couple of days, an appointment may be necessary where Dr. Talarico may add one or more of these additional modalities to your treatment program. Orthotic b, whether pre-fabricated or custom orthotic is used, these devices can help reduce the underlying structural abnormalities of the foot which have lead to the development of plantar fasciitis. These are often used to limit the recurrence of plantar fasciitis pain. Strapping, a special taping technique to help reduce the strain on the fascia. Injection therapy, in some instances injections are used to reduce the inflammation and reduce pain. Night Splint, this allows you to maintain an extended stretch on the plantar fascia while sleeping. Over time, this has shown to reduce the morning pain which some people experience. Removable Walking Cast, in some case of severe heel pain this may be used to keep your foot immobile for a few weeks allowing it to rest and heal. Physical Therapy may be recommended to aid in pain relief. At The Foot & Ankle Center, PC, Dr Talarico will often utilize two additional in-office modalities, EPAT and MLS Laser Therapy, which are very effective in treating most inflammatory conditions of the foot and ankle, including plantar fasciitis. Surgical Treatment It is rare to need an operation for heel pain. It would only be offered if all simpler treatments have failed and, in particular, you are a reasonable weight for your height and the stresses on your heel cannot be improved by modifying your activities or footwear. The aim of an operation is to release part of the plantar fascia from the heel bone and reduce the tension in it. Many surgeons would also explore and free the small nerves on the inner side of your heel as these are sometimes trapped by bands of tight tissue. This sort of surgery can be done through a cut about 3cm long on the inner side of your heel. Recently there has been a lot of interest in doing the operation by keyhole surgery, but this has not yet been proven to be effective and safe. Most people who have an operation are better afterwards, but it can take months to get the benefit of the operation and the wound can take a while to heal fully. Tingling or numbness on the side of the heel may occur after operation. heel cups for heel pain Prevention  Wearing real good, supportive shoes are a great way to avoid heel pain. Usually, New Balance is a good shoe to wear, just for everyday shoe gear. By wearing proper footwear and performing thorough stretches, athletes can help prevent frequent heel pain. If you are starting to get a little discomfort or pain in the feet or heel, know that pain is not normal. So if you are having pain, you should be proactive and visit our office. If you let heel pain get out of control you could run into several other problems. It is always suggested to visit a podiatrist whenever you are experiencing pain. Overview
 Morton?s neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton?s neuroma is 8 to 10 times greater in women than in men. Morton?s neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton?s neuroma is 8 to 10 times greater in women than in men.Causes Anything that causes compression or irritation of the nerve can lead to the development of a neuroma. One of the most common causes comes from wearing shoes that have a tapered toe box, or high-heeled shoes that cause the toes to be forced into the toe box and overload pressure onto the forefoot. An injury or trauma to the forefoot may also lead to a neuroma. People at a higher risk of developing a Neuroma include people with certain foot deformities, such as bunions or hammertoes. Certain foot types, such as flat feet (Pronation) More flexible feet, and woman after pregnancy. Symptoms There may be pain at the end of the push-off phase when walking or running, and this pain is generally worse when the client is wearing shoes as opposed to being barefoot. Clients may also report a relief of symptoms by massaging the foot, which may spread the metatarsal heads and mobilize the entrapped nerve. Diagnosis Diagnosis of Morton?s Neuroma typically involves a physical examination of the affected foot. Your health care provider will ask you about your symptoms and examine your feet and toes. He will manipulate your toes, pushing them from side to side and squeezing on the spaces in between. This physical exam will allow your health care provider to feel for any lumps that may be present under the soft tissue of your feet. Your health care provider may also listen for any clicking sounds that your bones may be making. Known as Muldor?s Sign, this clicking is common amongst sufferers of foot neuroma. Occasionally, an x-ray or MRI (magnetic resonance imaging) is performed to help rule out any breaks, sprains, or fractures in your foot. Non Surgical Treatment Common treatments involve wearing different shoes or using arch supports. Resting the foot, massaging the toes and using an ice pack may work for some people. A GP or a podiatrist (foot specialist) may also recommend anti-inflammatory painkillers or a course of steroid injections. Numbing injections, in which alcohol and a local anaesthetic are injected into the affected area of the foot, may also be effective. In extreme cases, when the condition does not respond to treatment, day case surgery may be needed.  Surgical Treatment Surgery for Morton's neuroma is usually a treatment of last resort. It may be recommended if you have severe pain in your foot or if non-surgical treatments haven't worked. Surgery is usually carried out under local anaesthetic, on an outpatient basis, which means you won't need to stay in hospital overnight. The operation can take up to 30 minutes. The surgeon will make a small incision, either on the top of your foot or on the sole. They may try to increase the space around the nerve (nerve decompression) by removing some of the surrounding tissue, or they may remove the nerve completely (nerve resection). If the nerve is removed, the area between your toes may be permanently numb. After the procedure you'll need to wear a special protective shoe until the affected area has healed sufficiently to wear normal footwear. It can take up to four weeks to make a full recovery. Most people (about 75%) who have surgery to treat Morton's neuroma have positive results and their painful symptoms are relieved. Prevention Women, particularly those who wear tight shoes, are at greatest risk for Morton?s neuroma. The best way to prevent the condition is to wear shoes with wide toe boxes. Tight, pointed shoes squeeze bones, ligaments, muscles and nerves. High heels may worsen the problem by shifting your weight forward. Over time, this combination can cause the nerves to swell and become painful.
Overview
 A bunion is an abnormal bump, or bony enlargement that forms at the base of your big toe. In the early stages, the bunion may be small and the side of your foot may be slightly swollen. As it progresses, the bump gets larger and becomes increasingly painful. Your big toe may point towards your other toes, rather than straight. Shoes may be uncomfortable to wear and add to the irritation of the joint. A bunion is an abnormal bump, or bony enlargement that forms at the base of your big toe. In the early stages, the bunion may be small and the side of your foot may be slightly swollen. As it progresses, the bump gets larger and becomes increasingly painful. Your big toe may point towards your other toes, rather than straight. Shoes may be uncomfortable to wear and add to the irritation of the joint.Causes Women traditionally have a higher rate of bunions, which is to be expected, since it is they who have traditionally worn shoes with high heels, a narrow toe box, or whatever fashion dictates from year to year. However, men can suffer from bunions as well, as can anyone for whom the right (or wrong) conditions exist, poor foot mechanics, improper footwear, occupational hazards, health and genetic predisposition. Finally, bunions have long been a condition associated with the elderly, and although they often appear in conjunction with inflammatory joint diseases such as arthritis (which is often associated with age), they can strike at any point in life, including adolescence. Symptoms With Bunions, a person will have inflammation, swelling, and soreness on the side surface of the big toe. Corns most commonly are tender cone-shaped patches of dry skin on the top or side of the toes. Calluses will appear on high-pressure points of the foot as thick hardened patches of skin. Diagnosis Your doctor can identify a bunion by examining your foot. Watching your big toe as you move it up and down will help your doctor determine if your range of motion is limited. Your doctor will also look for redness or swelling. After the physical exam, an X-ray of your foot can help your doctor identify the cause of the bunion and rate its severity. Non Surgical Treatment Treatment options vary depending on the severity of your bunion and the amount of pain it causes you. Early treatment is best to decrease your risk of developing joint deformities. Conservative treatment Nonsurgical treatments that may relieve the pain and pressure of a bunion include changing shoes. Wear roomy, comfortable shoes that provide plenty of space for your toes. Padding and taping. Your Podiatrist can help you tape and pad your foot in a normal position. This can reduce stress on the bunion and alleviate your pain.(Obviously pending on footwear selection). Medications. Acetaminophen (Tylenol, others) can control the pain of a bunion. Your doctor may suggest nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen (Advil, Motrin, others) or naproxen (Aleve), for relieving pain and reducing inflammation. Cortisone injections also can be helpful. But keep in mind that medications do not alleviate the actual cause of the pain. Physical therapy. The heating effect of ultrasound therapy or whirlpool baths can provide relief from the pain and inflammation of a bunion. Orthotics can help control abnormal movement of your foot, reducing your symptoms and preventing your bunion from getting worse. Over-the-counter arch supports can provide relief for some people, though others may require prescription orthotics.  Surgical Treatment In some very mild cases of bunion formation, surgery may only be required to remove the bump that makes up the bunion. This operation, called a bunionectomy, is performed through a small incision on the side of the foot immediately over the area of the bunion. Once the skin is opened the bump is removed using a special surgical saw or chisel. The bone is smoothed of all rough edges and the skin incision is closed with small stitches. It is more likely that realignment of the big toe will also be necessary. The major decision that must be made is whether or not the metatarsal bone will need to be cut and realigned as well. The angle made between the first metatarsal and the second metatarsal is used to make this decision. The normal angle is around nine or ten degrees. If the angle is 13 degrees or more, the metatarsal will probably need to be cut and realigned. Prevention Proper footwear may prevent bunions. Wear roomy shoes that have wide and deep toe boxes (the area that surrounds the toes), low or flat heels, and good arch supports. Avoid tight, narrow, or high-heeled shoes that put pressure on the big toe joint. Medicine will not prevent or cure bunions. Overview
Over-pronation, or flat feet, is a common biomechanical problem that occurs in the walking process when a person?s arch collapses upon weight bearing. This motion can cause extreme stress or inflammation on the plantar fascia, possibly causing severe discomfort and leading to other foot problems.  Causes Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should. Symptoms Common conditions seen with overpronation include heel pain or plantar fasciitis. Achilles tendonopathy. Hallus Valgus and/or bunions. Patellofemoral pain syndrome. Iliotibial band pain syndrome. Low back pain. Shin splints. Stress fractures in the foot or lower leg. Diagnosis Bunions, calluses and crooked toes may indicate alignment problems. So, it is important to ascertain the condition of a client's toes. Check the big toe to determine if the first joint of the toe is swollen, has a callus or bunion, and/or looks as though it abducts (i.e., hallux valgus) rather than pointing straight ahead. Also, look to see if the lesser toes seem to "curl up" (i.e., the person has hammer or claw toes). This may be indicative of damage to, or inflexibility of the plantar fascia caused by excessive flattening of the foot.  Non Surgical Treatment Get a gait analysis of your running style, this will highlight if you overpronate, oversupinate or have a neutral gait. Most podiatrists, physio's and sports therapists will offer this service, as do some specialist sports shops. Find a clinic. If you overpronate, get orthotics with extra medial support. Many running shoes have a harder material on the inside of the midsole (the thick hard foam part of the running shoe). This means the inside of the shoe will be compressed less under load and support the inside of the foot preventing it from rolling in or flattening. For people with considerable overpronation, another option is to have an orthotic device fitted. Orthotic insoles come in many types and prices. Some are pre-molded and can be bought off the shelf. These are ok for the majority of problem feet. However some cases may require specially casted orthotics from a relevant sports injury therapist or podiatrist. Prevention With every step we take, we place at least half of our body weight on each foot (as we walk faster, or run, we can exert more than twice our body weight on each foot). As this amount of weight is applied to each foot there is a significant shock passed on to our body. Custom-made orthotics will absorb some of this shock, helping to protect our feet, ankles, knees, hips, and lower back. Overview
n the growing child there are a number of different ways that bones grow. In the calcaneus (heel bone), growth comes from two separate growth plates. The lesser of the two growth plates is called the apophysis. The apophysis of the calcaneus is located between the back and the bottom of the heel at that spot that hits the ground each time we take a step. The Achilles tendon, which is the most powerful tendons in our body, attaches to the proximal aspect of the apophysis. The plantar fascia attaches to the distal aspect of the apophysis. Both the Achilles tendon and plantar fascia place traction, or pulling on the growth plate and contribute to inflammation of the secondary growth plate called apophysitis. The calcaneal apophysis is very apparent on x-ray and continues to grow until approximately age 12 in girls and age 15 in boys. Causes Growth plates, also called epiphyseal plates, occur at the end of long bones in children who are still growing. These plates are at either end of growing bones, and are the place where cartilage turns into bone. As children grow, these plates eventually become bone (a process called ossification). During a growth spurt, the bone in the heel may outpace the growth of the muscles and tendons that are attached to the heel, such as the Achilles tendon. During weight bearing, the muscles and tendons begin to tighten, which in turn puts stress on the growth plate in the heel. The heel is not very flexible, and the constant pressure on it begins to cause the symptoms of Sever?s disease. Sever?s disease is common, and it does not predispose a child to develop any other diseases or conditions in the leg, foot, or heel. It typically resolves on its own. Symptoms If your child is suffering from this disease they will be experiencing pain and tenderness in the back of their foot. This soreness can also extend to the sides of the feet. Other sure signs of this disorder include swelling and sensitivity to touch. Because of the amount of discomfort, your child may find it difficult to walk or run. Pay attention to the way your child is walking. If you notice unusual posture or abnormal gait they may be avoiding placing pressure on the heel. These symptoms typically become apparent during activity and exercise or directly following it. If your child is indicating pain in their heel, schedule an appointment with us today. Diagnosis The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone. Non Surgical Treatment Initially, Sever?s Disease is treated with rest, anti-inflammatory medication and softer shoes. Ice followed by heat is a common practice and heel cup orthotics have worked wonders for our young patients in the past. It can take anywhere from a few weeks to a year for these growth plates to naturally close - at which point Sever?s Disease disappears. Even though the condition does heal on its own, athletes are encouraged to seek treatment, rather than push through the pain. Simply ?dealing with it? and continuing to play sports despite the injury could lead to an impaired gait, a strained hip or a knee injury. Stretches to strengthen the leg muscles, leg compression wraps and over-the-counter acetaminophen or ibuprofen are also recommended treatments. In very rare cases, a podiatrist may recommend wearing a cast for two to twelve weeks. Overview
Pain or strain in your foot arches is a common sports injury and often linked to inflammation of the plantar fascia, the shock absorption ligament along the bottom of each foot. The pain can also highlight underlying issues to do with the structure of your arches.  Causes Recent research has found a link with changes to the tendon in the foot and an increase in a type of protein called proteolytic enzyme. These enzymes can break down some areas of the tendon, weakening it and causing the foot arch to fall. Similar changes are also seen in other conditions, such as Achilles tendonitis. This could have important implications for treating flat feet because medication that specifically targets these enzymes could provide an alternative to surgery. However, further research is needed and this type of treatment is thought to be about 10 to 15 years away. Symptoms The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused. Diagnosis A professional therapist may use tinels test to diagnose tarsal tunnel syndrome. This involves tapping the nerve just behind the medial malleolus or bony bit of the ankle with a rubber hammer. Pain indicates a positive test. Sometimes it is initially mistaken for plantar fasciitis which also causes pain from the inside heel and throughout the arch of the foot. Neural symptoms (such as tingling or numbness) as well as the location of tenderness when touching the area should help to easily distinguish between the conditions. Non Surgical Treatment The adult acquired flatfoot is best treated early. There is no recommended home treatment other than the general avoidance of prolonged weightbearing in non-supportive footwear until the patient can be seen in the office of the foot and ankle specialist. In Stage I, the inflammation and tendon injury will respond to rest, protected ambulation in a cast, as well as anti-inflammatory therapy. Follow-up treatment with custom-molded foot orthoses and properly designed athletic or orthopedic footwear are critical to maintain stability of the foot and ankle after initial symptoms have been calmed. Once the tendon has been stretched, the foot will become deformed and visibly rolled into a pronated position at the ankle. Non-surgical treatment has a significantly lower chance of success. Total immobilization in a cast or Camwalker may calm down symptoms and arrest progression of the deformity in a smaller percentage of patients. Usually, long-term use of a brace known as an ankle foot orthosis is required to stop progression of the deformity without surgery.  Surgical Treatment In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions. Stretching Exercises Calf Raises. Strengthens the tendons in your heels and calf muscles, which support your arch. Raise up on the balls of your feet as high as possible. Slowly lower down. Do three sets of 10 reps. Progress to doing the raises on stairs (with heels hanging off), and then to single-leg raises. Step Stretch. Improves flexibility in your Achilles tendon and calf-when these areas become tight, the arch gets painfully overloaded. Stand at the edge of a step, toes on step, heels hanging off. Lower your heels down, past the step, then raise back up to the start position. Do three sets of 10 reps. Doming. Works the arch muscles and the tibialis posterior (in the calf and foot) to control excess pronation. While standing, press your toes downward into the ground while keeping the heel planted, so that your foot forms an arch (or dome). Release, and do three sets of 10 reps on each foot. Toe Spread and Squeeze. Targets the interossei muscles of the foot, which support the arch. While sitting, loop a small resistance band around your toes. Spread toes; release. Then place a toe separator (used at nail salons) in between toes. Squeeze toes in; release. Do three sets of 10 reps of each exercise on both feet. Towel Curls. Works the toe-flexor muscles that run along your arch to increase overall foot strength. Lay a small hand towel on the floor, and place one foot on the towel. Using just your toes, scrunch the towel toward you, hold, then slowly push the towel away from you back to start position. Do three sets of 10 reps on each foot.
Overview
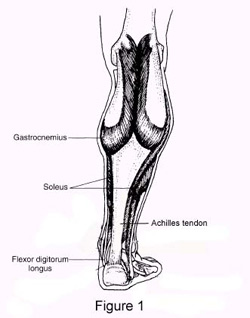 Your Achilles tendon is a large band of tissue in the back of your ankle. It connects your calf muscles to your heel bone. The tendon helps you point your foot downward, rise on your toes, and push off when you walk. You use it almost every time you move. But repeated stress can make the tendon more prone to injury. It may become inflamed and develop small tears (tendonitis). A complete tear through the tendon is known as an Achilles tendon rupture. Your Achilles tendon is a large band of tissue in the back of your ankle. It connects your calf muscles to your heel bone. The tendon helps you point your foot downward, rise on your toes, and push off when you walk. You use it almost every time you move. But repeated stress can make the tendon more prone to injury. It may become inflamed and develop small tears (tendonitis). A complete tear through the tendon is known as an Achilles tendon rupture.Causes People who commonly fall victim to Achilles rupture or tear include recreational athletes, people of old age, individuals with previous Achilles tendon tears or ruptures, previous tendon injections or quinolone use, extreme changes in training intensity or activity level, and participation in a new activity. Most cases of Achilles tendon rupture are traumatic sports injuries. The average age of patients is 29-40 years with a male-to-female ratio of nearly 20:1. Fluoroquinolone antibiotics, such as ciprofloxacin, and glucocorticoids have been linked with an increased risk of Achilles tendon rupture. Direct steroid injections into the tendon have also been linked to rupture. Quinolone has been associated with Achilles tendinitis and Achilles tendon ruptures for some time. Quinolones are antibacterial agents that act at the level of DNA by inhibiting DNA Gyrase. DNA Gyrase is an enzyme used to unwind double stranded DNA which is essential to DNA Replication. Quinolone is specialized in the fact that it can attack bacterial DNA and prevent them from replicating by this process, and are frequently prescribed to the elderly. Approximately 2% to 6% of all elderly people over the age of 60 who have had Achilles ruptures can be attributed to the use of quinolones. Symptoms Whereas calf strains and tendonitis may cause tightness or pain in the leg, Achilles tendon ruptures are typically accompanied by a popping sensation and noise at the time of the injury. In fact, some patients joke that the popping sound was loud enough to make them think theyd been shot. Seeing a board-certified orthopedic surgeon is the best way to determine whether you have suffered an Achilles tendon tear. Diagnosis Your caregiver will ask what you were doing at the time of your injury. You may need any of the following. A calf-squeeze test is used to check for movement. You will lie on your stomach on a table or bed with your feet hanging over the edge. Your caregiver will squeeze the lower part of each calf. If your foot or ankle do not move, the tendon is torn. An x-ray will show swelling or any broken bones. An ultrasound uses sound waves to show pictures of your tendon on a monitor. An ultrasound may show a tear in the tendon. An MRI takes pictures of your tendon to show damage. You may be given dye to help the tendon show up better. Tell the caregiver if you have ever had an allergic reaction to contrast dye. Do not enter the MRI room with anything metal. Metal can cause serious injury. Tell the caregiver if you have any metal in or on your body. Non Surgical Treatment Pain medicines can help decrease pain and swelling. A cast may be needed for 2 months or more. Your foot will be positioned in the cast with your toes pointing slightly down. Your caregiver will change your cast and your foot position several times while the tendon heals. Do not move or put weight on your foot until your caregiver tells you it is okay. A leg brace or splint may be needed to help keep your foot from moving while your tendon heals. Heel lifts are wedges put into your shoe or cast. Heel lifts help decrease pressure and keep your foot in the best position for your tendon to heal. Surgery may be needed if other treatments do not work. The edges of your tendon may need to be stitched back together. You may need a graft to patch the tear. A graft is a piece of another tendon or artificial material.  Surgical Treatment Debate remains regarding the best form of treatment for a ruptured Achilles tendon. The 2 options are:immobilisation or operation. A recent meta-analysis of scientific studies showed that compared to immobilisation, an operation reduces the risk of re-rupture and allows a quicker return to work. An operation is not without risk and these must be balanced against the benefit of a lower re-rupture rate. Both treatments involve immobilisation for 8 weeks. Prevention To help prevent an Achilles tendon injury, it is a good practice to perform stretching and warm-up exercises before any participating in any activities. Gradually increase the intensity and length of time of activity. Muscle conditioning may help to strengthen the muscles in the body. |
